Anaesthetic Equipment
Anaesthetic Equipment
Breathing Systems
Paediatric anaesthetic equipment should:
- Have minimal resistance to breathing
- Have minimal dead space
- Be light (not bulky)
- Be simple to use
- Provide humidification of inspired gases.
The following systems are described
Jackson Rees modification
Draw-over system with Paedivalve
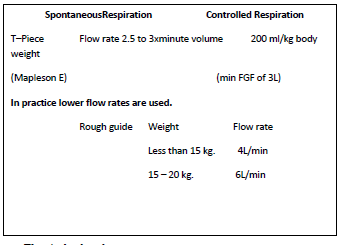
Ayre's T-Piece
This is a simple metal T Tube (Mapleson E circuit). Disposable plastic versions are available. It connects to the patient via an endotracheal tube connector.It connects to an extension tube which acts as a reservoir and then opens into the atmosphere.It connects to a gas source, e.g. an anaesthetic machine. Nitrous oxide, oxygen and inhalational agents such as halothane may be fed into the T-piece. Adjustment of the fresh gas flow can prevent rebreathing of expired air. Accumulation of CO2 is prevented. Intermittent occlusion of the open end allows controlled ventilation.
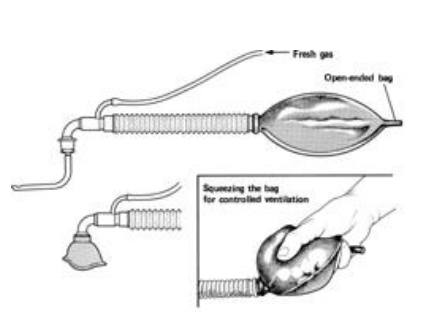
Jackson Rees Modification of Ayre's T-Piece
Jackson Rees added an open-ended 500 ml bag to the expiratory limb. This makes controlled ventilation possible on application of continuous positive airway pressure (CPAP). The movement of the bag indicates the patient's respiratory activities during spontaneous respiration. During spontaneous ventilation the fresh gas flow should be 2-3 times the minute volume. During controlled ventilation the flow rate can be 200 ml/kg with a minimum flow of 3L/min. (Some degree of rebreathing may occur at these flow rates but it is compensated for by hyperventilation).
Advantages of a T-Piece
- The dead space is minimal, equal to the volume of the apparatus between the point of entry of the fresh gases and the patient.
- Resistance to flow is minimal because there are no valves.
- Rebreathing is virtually eliminated if the prescribed fresh gas flows are used.
- It is light.
- It is relatively cheap.
- It is simple.
Disadvantages of the T-Piece
- It needs a high flow rate. This makes it expensive to use, so it is a wasteful and expensive system to use where anaesthetic gases and agents are in short supply or for children > 25kg.
- The gases inhaled are dry unless they are artificially humidified.
- Theatre pollution becomes an even greater problem with the T piece. A scavenging system is necessary.
Draw-Over System With Paedivalve
This arrangement is used for children under 15kg and is a low cost draw-over technique.
The paedivalve is a non-rebreathing valve (like a miniature Ambu E valve) and is used in conjunction with paediatric bellows replacing the standard adult bellows on the OIB base or with a paediatric self-inflating resuscitation bag. This delivery system can then be used with the OMV, using halothane and entraining oxygen from an oxygen concentrator.

In summary
The circle absorber This is described in detail under anaesthetic machines in module 2 . The adult circle can be used in children over 25 kg in weight or over 5 years of age. This would be reasonable for controlled ventilation. The decision to use controlled ventilation would be made on surgical indications. It can be used for spontaneous respiration in older children above 35 kg in weight
Other Equipments for Paediatric Anesthesia
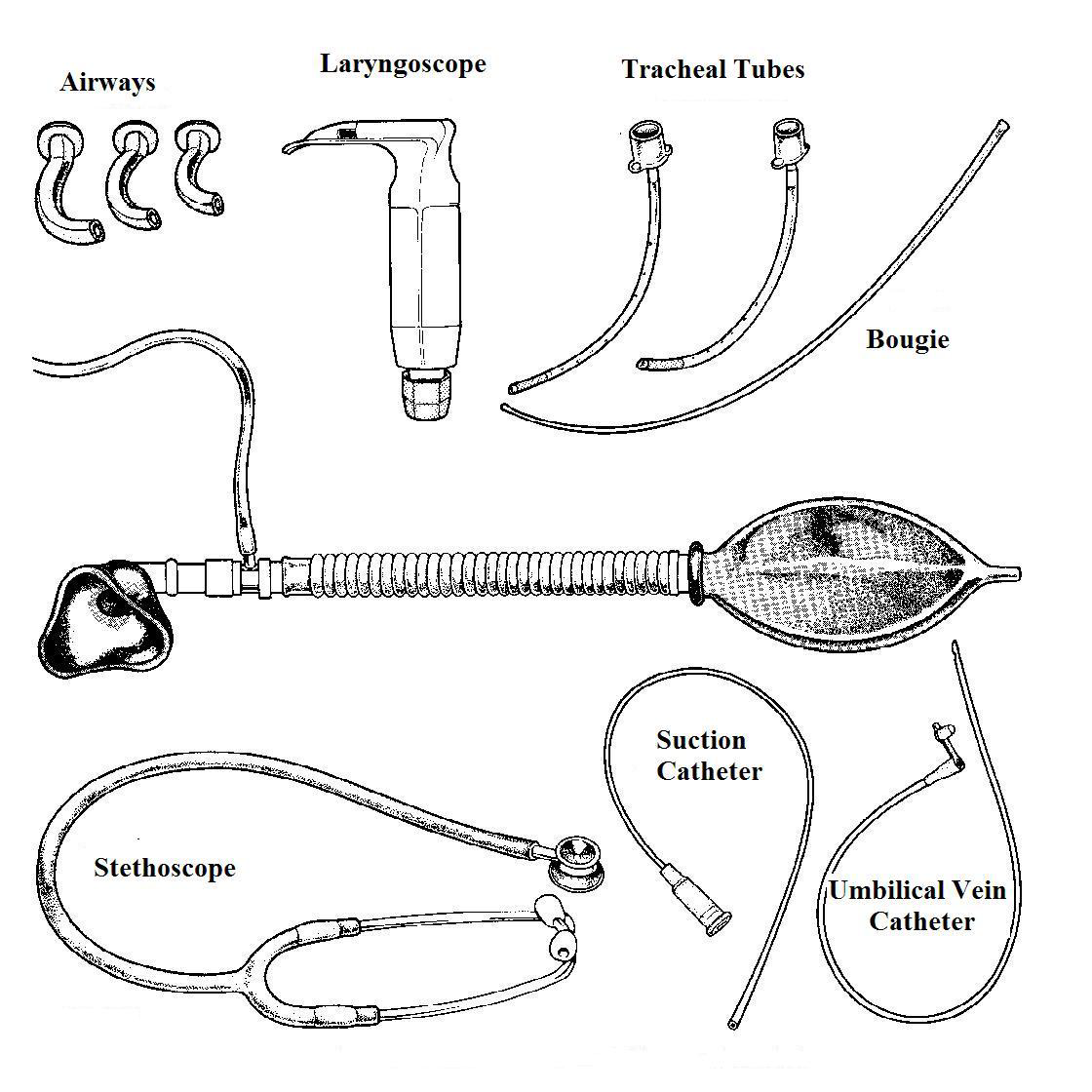
LaryngoscopesA wide range of laryngoscopes is available for pediatric use. The straight blade laryngoscope is useful in neonates and infants (up to the age of 1 year). The curved blade may be used for children above the age of 1 year but the choice of the blade depends on the anesthetist's preference. The straight blade laryngoscope is introduced under the epiglottis. It is especially suitable in neonates who have a floppy U shaped epiglottis but be careful of vagal reflexes. The curved blade is inserted in front of the epiglottis, between the epiglottis and the base of the tongue.
Endotracheal tubes and connectors
Polyvinyl chloride (PVC) tubes : are available for paediatric use as for adults. The tubes are non-irritant and though disposable, may be re-used after cleaning. Uncuffed tracheal tubes are usually used in children to prevent problems with sub-glottic oedema or stenosis.
A guide to uncuffed tracheal tube size is:
| Weight or Age | Tracheal Tube Size (Internal Diameter, mm) |
|---|---|
| >2kg | 2.5 |
| Newborn | 3.0-3.5 |
| 3 months - 1 year | 4.0 |
| Over 2 years | Age/4 + 4 |
Appropriately sized cuffed tubes may be considered in children of all ages but especially those at risk of aspiration or with stiff, poorly compliant lungs. The size of cuffed tube is one size smaller than an uncuffed tube (age/4 + 3). Care should be taken to avoid over-inflation of the cuff.In all cases, a tracheal tube one size above and below that calculated should be available.
RAE tubes: These are PVC tubes with a bend in them suitable for both nasal and oral use.
Latex or reinforced tubes: are incompressible, almost unkinkable but floppy and accidental extubation is possible. Latex deteriorates rapidly after sterilisation.
Cole (or Foregger or Rusch tubes). These have an expanded oral part which prevents insertion too far down. The smallest size can be used if the other tubes are too large. The shoulder on the Cole tube is said to prevent insertion too far down the trachea but it may act as a laryngeal dilator and cause serious laryngeal oedema. This type of tube is easy to insert but should not be left in place for more than a few hours because of this hazard.
The tubes most recommended are PVC and RAE tubes.
Masks
The Rendell-Baker mask was designed to fit the contours of the face and reduce dead space. In the smallest of these masks the dead space is 4 ml. They are available in sizes 0, 1, 2, 3 and 4. Cushioned clear plastic facemasks (when available) are the current standard as they are easy to use, non-threatening to the child and regurgitation is easily detected.
Airways
The Guedel oropharyngeal airways are most commonly used. They are made of PVC or firm rubber. A metal insert prevents obstruction of the airway by the patient biting on it. The Guedel airway is available in sizes 000 to 4. The airway is sized from the distance from the incisors to the angle of the jaw. It is important to use the correct sized airway.