Palpation of the abdomen
Palpation means feeling the abdomen with your hands in specific positions, or moving them in particular ways, using certain levels of pressure. Ask the mother to lie down on her back and bend her legs at the knees, with her feet flat on the bed. You need to be able to move around her: sometimes you will be palpating her abdomen while standing at her feet and looking up her body towards her head; sometimes you will be standing behind her and facing her feet; and sometimes you will stand beside her.
Can you recall the purposes of abdominal palpation in a woman in labour? (They are the same as during the pregnancy; see Antenatal Care Module, Study Session 11.)
Palpation helps you to assess the size of the fetus, its presentation (which part of the baby will 'present' at the cervix during delivery), and its position relative to the mother's body (e.g. is it facing towards her front or her back).
There are four palpations of the abdomen, which are commonly referred to by midwives and doctors as Leopold's manoeuvres. You need to do them in the correct sequence.
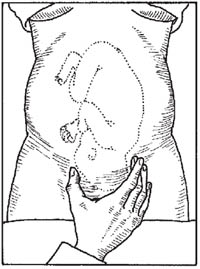
First Leopold's manoeuvre: fundal palpation
Fundal palpitation means palpating the dome-shaped upper part of the uterus, called the fundus. During antenatal care, you should have been measuring the length of the uterus from the mother's pubic bone to the fundus, and comparing this with the baby's gestational age to see if it was growing normally. The purpose of palpating the fundus in a woman in labour is to discover how the baby is lying in the uterus.
Use the palms of both hands to palpate on either side of the fundus, with your fingers quite close together (see Figure 2.4). Feel whether the top part of the uterus is hard and rounded or soft and irregular. If the shapes feel soft and irregular and they don't easily move under gentle pressure from your hands, then the baby's buttocks are occupying the fundus (as in Figure 2.4) and it is 'head-down'. This is cephalic presentation (cephalic means head). There are several different cephalic presentations, which you will learn about in Study Session 8. The most common, and the easiest for the baby to be born, is called the vertex presentation.
If you can feel a hard, round shape in the fundus, this is the baby's head. In a woman who is already in labour, this means the baby is in the breech presentation (the buttocks are the presenting part). It is safest to refer a woman whose baby is in the breech position because the birth is likely to be more difficult and the risk of complications is higher. If the fundus feels 'empty', the baby may be lying diagonally or transversely across the uterus. The second manoeuvre will help to clarify this.
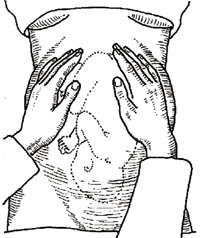
Second Leopold's manoeuvre: lateral palpation
The second manoeuvre helps you to discover the fetal lie: is the baby lying longitudinally (straight), obliquely (diagonally across the uterus), or transversely (horizontally)? The longitudinal lie is normal (see Figures 2.4 and 2.5). A transverse lie in labour should be referred urgently; the baby cannot be born through the vagina in this position and may need caesarean surgery to deliver it.
Place your hands on either side of the middle of her abdomen. Push gently with one hand while holding the other hand firm to steady the uterus; alternate the pressure between your two hands. If you feel the round, hard shape of the baby's head at one side, and the fundus feels empty, it may be a transverse lie and you should refer the mother urgently.
The second manoeuvre also helps to determine whether the baby is facing inwards or outwards. Note the regularity of the shapes you can feel under your hands. If you can feel a large smooth shape under one hand, this is probably the baby's back, which means it is facing inwards (Figure 2.5a). In this starting position it is easier for the baby to begin the seven cardinal movements you learned about in Study Session 1 (look back at Figure 1.3). If you can feel small irregular 'lumps' under your hands, these are probably the baby's feet, knees and elbows and it is facing outwards (Figure 2.5b). It is not so easy for it to rotate as it passes down the birth canal from this starting position.
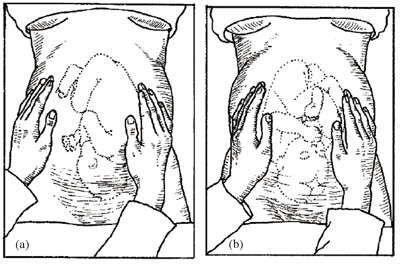
Third Leopold's manoeuvre: deep pelvic palpation
The third manoeuvre helps to confirm your earlier findings about the fetal presentation—is it cephalic or breech?
What is cephalic presentation?
The fetus is head down with its buttocks occupying the fundus (the upper part of the uterus).
Face the woman's feet and place your hands on the lower part of her abdomen, with your fingers gently pressing inwards just above her pubic bone (see Figure 2.6). You are feeling for the presenting part of the fetus as it engages with the cervix. If it is hard and round, the presentation is cephalic; if it is softer and irregular, suspect a breech presentation.
You learned directional terms in anatomy, like anterior and posterior, in Study Session 3 of the Antenatal Care Module, Part 1.
You may also be able to confirm your findings from the second manoeuvre about whether the baby has its back towards you or not. If it does, this is called the occipito-anterior position: the occiput is the point at the back of the fetal skull, which is lying in the anterior position (Figure 2.6a), that is, towards the front of the mother. A baby that presents in the occipito-posterior position (Figure 2.6b) may encounter more difficulties during delivery.
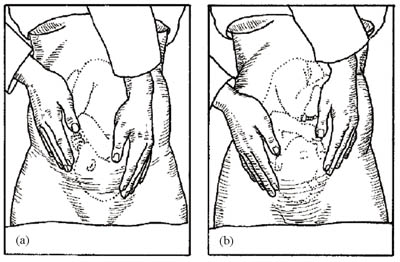
Fourth Leopold's manoeuvre: Pawlick's grip
The purpose of the fourth manoeuvre (also known as Pawlick's grip) is to help determine whether the fetal head (in a cephalic presentation) has descended into the mother's pelvis and engaged in the cervix. (Engagement was explained in Study Session 1.) The extent of engagement is estimated by how many fingers you can grip the fetal head with (Figure 2.7). If all five fingers can grip the fetal head just above the mother's pubic bone, the head is not yet engaged. When you can only grip it with the width of two fingers, the head is engaged.